
- Important Facts
- Data Views
- lifetime prevalence among adults aged 18 and older, Utah and U.S., 2021-2022
- by disability, Utah adults aged 18 and older, 2022
- Utah and U.S., 2001-2022
- by age and sex, Utah, 2022
- by ethnicity, Utah, 2021-2022
- by race, Utah, 2021-2022
- by educational level, Utah, 2021-2022
- by income level, Utah, 2021-2022
- by local health district, Utah 2021-2022 and U.S. 2022
- by local health district, all ages, Utah, 2022
- by Utah Small Area, 2018-2022
- Related Indicators
- Available Services
- Other Resources & Links
- Full Report
- Main XML Data
- Values XML Data



Health Indicator Report of Asthma: Adult Prevalence
Asthma is a serious personal and public health issue that has far reaching medical, economic, and psychosocial implications. The burden of asthma can be seen in the number of asthma-related medical events, including emergency department visits, hospitalizations, and deaths.
Adult asthma prevalence by local health district, Utah 2021-2022 and U.S. 2022
Prevalence of current asthma by local health district, Utah, 2021-2022
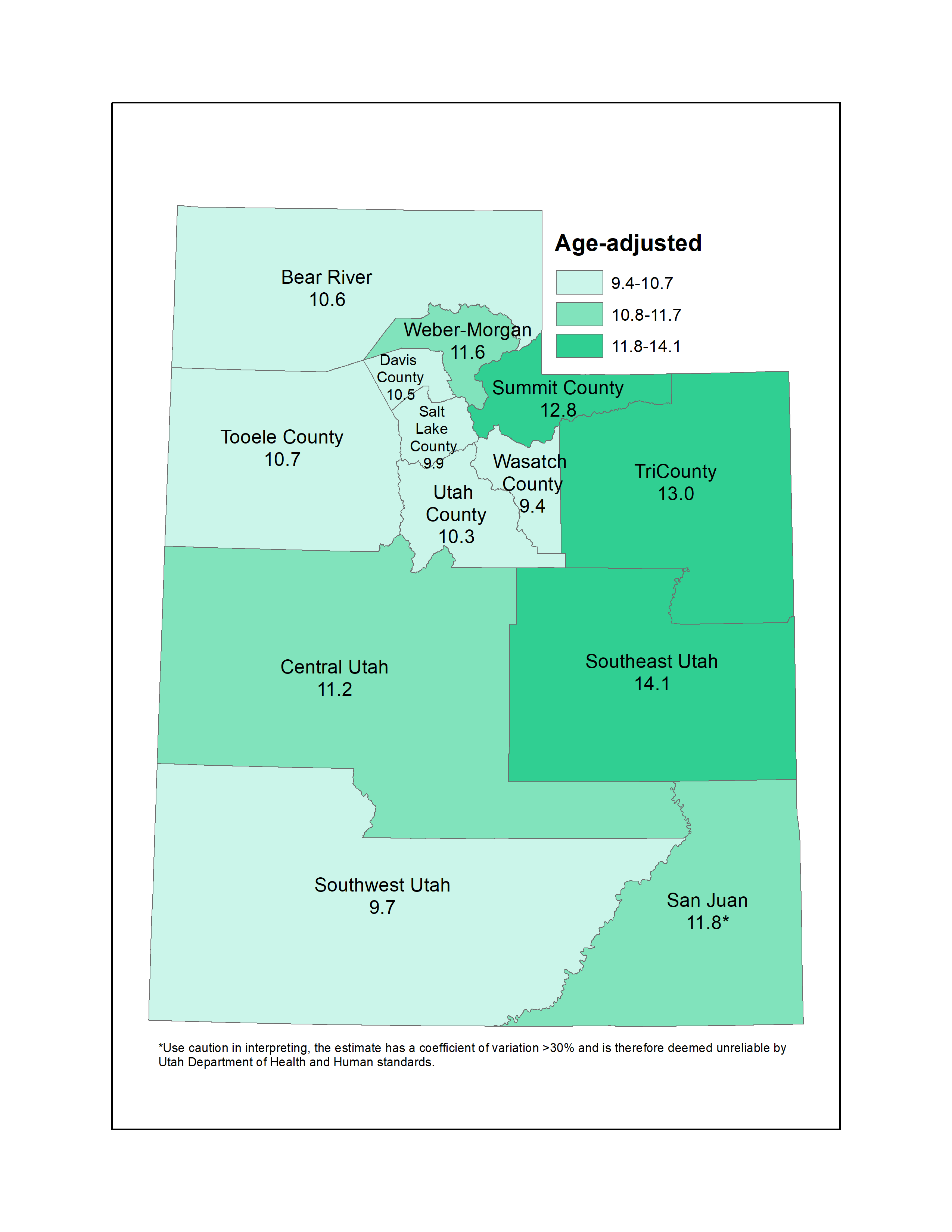
This map was made using an interval break method called "natural breaks" where classes are based on natural groupings inherent in the data.
Notes
*Use caution in interpreting. The estimate has a coefficient of variation >30% and is therefore deemed unreliable by Utah Department of Health and Human Services standards. Percentages have been age-adjusted to the U.S. 2000 standard population.Data Sources
- Utah Department of Health and Human Services Behavioral Risk Factor Surveillance System (BRFSS) [https://ibis.utah.gov/ibisph-view/query/selection/brfss/BRFSSSelection.html]
- Behavioral Risk Factor Surveillance System Survey Data, US Department of Health and Human Services Centers for Disease Control and Prevention (CDC).
Data Interpretation Issues
Beginning in 2011, BRFSS data include both landline and cell phone respondent data along with a new weighting methodology called iterative proportional fitting, or raking. This methodology utilizes additional demographic information (such as education, race, and marital status) in the weighting procedure. Both of these methodology changes were implemented to account for an increased number of U.S. households without landline phones and an under-representation of certain demographic groups that were not well-represented in the sample. More details about these changes can be found at: [https://ibis.utah.gov/ibisph-view/pdf/opha/resource/brfss/RakingImpact2011.pdf].Definition
Adults aged 18+ (unless otherwise noted), who reported having been told by a doctor that they have asthma and who currently have asthma.Numerator
Total number of respondents answering "yes" to both of the BRFSS asthma core questions:[[br]] 1. Have you ever been told by a doctor, nurse, or other health professional that you had asthma?[[br]] 2. Do you still have asthma?Denominator
Includes all survey respondents ages 18 years and older except those with missing, don't know, or refused answers to the core asthma questions.How Are We Doing?
Adult asthma rates show no sign of declining in Utah or in the U.S. In Utah and the U.S., adult asthma prevalence is higher for women than men in almost every age category.How Do We Compare With the U.S.?
In 2022, Utah had a higher adult asthma prevalence rate when compared to the national average (10.9% vs. 10.0%).What Is Being Done?
The Utah Asthma Program (UAP) works with the Utah Asthma Task Force and other partners to maximize the reach, impact, efficiency, and sustainability of comprehensive asthma control services in Utah. This is accomplished by providing a seamless alignment of asthma services across the public health and health care sector, ensuring that people with asthma receive all of the services they need. The UAP focuses on building program infrastructure and implementing strategies that improve asthma control, reduce asthma-related emergency department visits and hospitalizations, and reduce health care costs. Program infrastructure is strengthened through a focus on strategies to create and support a comprehensive asthma control program, these strategies include: strengthening leadership, building strategic partnerships, and using strategic communication, surveillance, and evaluation. In addition, the UAP implements strategies outlined in the Centers for Disease Control and Prevention (CDC) EXHALE technical package to improve asthma control. The six strategy areas outlined in the EXHALE technical package are:[[br]] 1. Education on asthma self-management.[[br]] 2. e-Xtinguishing smoking and secondhand smoke.[[br]] 3. Home visits for trigger reduction and asthma self-management.[[br]] 4. Achievement of guidelines-based medical management.[[br]] 5. Linkages and coordination of care across settings.[[br]] 6. Environmental policies or best practices to reduce asthma triggers from indoor, outdoor, and occupational sources. These strategies are expected to improve asthma control and quality of life by increasing access to health care and increasing coordination and coverage for comprehensive asthma control services both in the public health and health care sectors. Specifically, these strategies include identifying people with poorly controlled asthma, linking them to health care providers and NAEPP EPR-3 guidelines-based care, educating them on asthma self-management strategies, providing a supportive school environment, and referring to or providing home trigger reduction services for those who need them.Available Services
A list of Utah Asthma Program services for clinicians, community health workers, and people with asthma can be found at [https://asthma.utah.gov/]Health Program Information
Utah Asthma Program website: [https://asthma.utah.gov/] CDC EXHALE package: [https://www.cdc.gov/national-asthma-control-program/php/exhale/index.html]
Page Content Updated On 08/06/2024,
Published on 09/24/2024
